
Serum
nmol/L
Progesterone is a steroid hormone produced primarily by the corpus luteum in non pregnant women and by the placenta beginning the second trimester of pregnancy. Serum progesterone measurements are used to confirm the occurrence of ovulation and to assess corpus luteum function. Serial measurements can help to define the day of ovulation. Progesterone levels are useful in assessing ovarian response to therapy with hCG, hMG, FSH/LHRH, or clomiphene. Progesterone levels, together with the rate of change of serum hCG, help to distinguish normal intrauterine gestation from ectopic pregnancy of inevitable abortion.
Serum progesterone levels follow a cyclic pattern in non pregnant women. Ovarian production of progesterone is low during the first (follicular) phase of the menstrual cycle. Serum level is often below 1 ng/mL. After the luteinizing hormone (LH) surge at the time of ovulation, the progesterone level rises for 4 or 5 days. Serum levels may reach a peak of 20 nmol/l and then gradually decrease prior to the onset of menses. In adult males and prepubertal females, serum concentrations are normally < 1nmol/L. Progesterone remains at a constant low level in post menopausal women.
Serum progesterone levels increase during pregnancy. Progesterone is first produced by the corpus luteum that is stimulated by a viable pregnancy. During the first 8 to 10 weeks of gestation, concentrations change only slightly. Between gestational weeks 10 and 11, the placenta becomes the primary source of production and progesterone levels steadily rise. If pregnancy fails, progesterone levels fall. Measurement of serum progesterone during pregnancy is helpful in identifying ectopic and nonviable pregnancies. Progesterone levels >25 nmol/L exclude the diagnosis of an ectopic pregnancy, obviating the need for further testing. A single progesterone level of 5 nmol/L or less is indicative of a nonviable pregnancy regardless of location. .
Progesterone and 17 alpha-hydroxyprogesterone are weak androgens. Progesterone is increased in congenital adrenal hyperplasia due to 21-hydroxylase, 17-hydroxylase, and 11-beta hydroxylase deficiency. The following conditions are associated with abnormal progesterone levels:
| Test usage | |
| Abnormal Secretion | premenstrual tension irregular endometrium shedding membranous dysmenorrhea luteal insufficiency |
| Increased Levels | hyperthecosis luteoma congenital adrenal hyperplasia |
| Decreased Levels | Anovulatory cyles toxemia of pregnancy placental insufficiency |

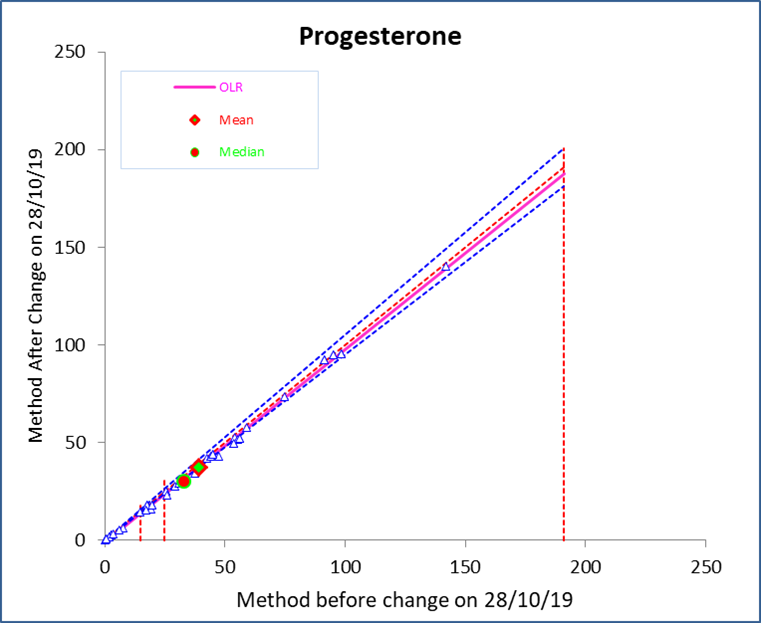
| Progesterone concentration (nmol/L) | Number Tested: | Mean bias (U/mL): | Bias % | |||
| Low: | to | 15 | 10 | -0.36 | -13.7 | |
| Mid: | 16 | to | 25 | 4 | -1.58 | -9.0 |
| High: | 26 | to | 191 | 21 | -2.43 | -5.6 |
Due to an equipment upgrade, the results reported for progesterone may be 6-14% lower than those reported before 28/10/19. Clinical cut-offs have not changed.
Local test
Same working days
Can be added on to an existing request up to 4 days following sample receipt
Specimen Labelling Procedure


8210
